
Ovarian torsion is the rotation of the ovary and the ligaments that hold it in place by surrounding organs. It is important to recognize the symptoms immediately and see a doctor at the first sign. Ovarian tissue can suffer irreversible damage if blood flow is interrupted for a long time.
Surgical intervention is urgently needed and time becomes a critical factor to save the ovary and prevent further complications. Read the article and find out how ovarian torsion manifests, why it occurs and how it is treated.
What is ovarian torsion?
Ovarian torsion is a gynecological emergency characterized by the twisting of the ovary and sometimes the fallopian tube around its ligaments. This twisting blocks blood flow to the ovary, leading to ischemia and necrosis if not treated quickly.
The condition occurs most commonly in young women of childbearing age , but it can occur at any age. Because of the risk of permanent damage to the ovary, ovarian torsion requires prompt diagnosis and emergency surgical treatment.
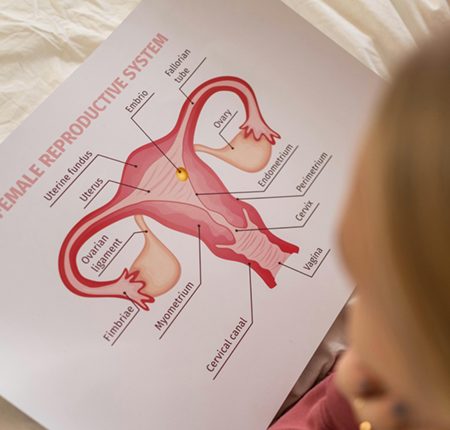
To better understand what's happening, think about how your reproductive organs are positioned in your body.
The two ovaries are located on either side of the uterus, attached by thin ligaments that maintain their position and also give them a certain mobility. Through these ligaments pass the blood vessels that nourish the ovary. When the ovary twists around its axis, these vessels are compressed and blood circulation is interrupted. Without enough oxygen, the ovarian tissue is quickly damaged.
This is why ovarian torsion is a medical emergency. The sooner surgery is performed, the better the chances of saving the ovary and ovarian function. The longer the procedure is delayed, the greater the risk of peritonitis (infection in the ovarian cavity) and necrosis (death of the ovary).
How does ovarian torsion occur?
Ovarian torsion occurs when the ovary twists around the structures that support it. The twisting can be complete or only partial, and in the long term can lead to peritonitis or loss of the ovary if not treated surgically.
Torsion can happen suddenly, on one side, and is generally accompanied by intense pain and vomiting.

Mechanism of ovarian torsion
When the ovary rotates around the axis formed by its supporting ligaments, the first function affected is venous circulation. This leads to congestion and swelling of the ovary. As the twisting persists, arterial circulation is also compromised.
The lack of oxygen and nutrients causes ischemia, which means the ovary is no longer supplied with blood. If the situation is not corrected quickly with surgery, necrosis of the ovarian tissue can occur.
Anatomy involved in ovarian torsion
The ovaries are located laterally to the uterus and are attached by thin ligaments that maintain their position, but also provide them with a certain level of mobility. Under certain conditions, this mobility can favor ovarian torsion.
Laxity of the ligaments or the presence of an enlarged ovarian cyst increase the risk of torsion because they alter the weight and stability of the ovary.
There are also situations where the twisting occurs not only in the ovary, but also in the adjacent fallopian tube (the thin tube that connects the ovary to the uterus). This situation is known as adnexal torsion and refers to the rotation of the fallopian tube around its axis.
Causes and risk factors for ovarian torsion
There are several anatomical and physiological factors that can influence the position and stability of the ovary, thus favoring the occurrence of ovarian torsion. Among the causes that can lead to ovarian rotation are:
- The presence of an ovarian cyst or tumor that can cause the ovary to shift and twist, especially in the case of ovarian cyst torsion.
- Pregnancy and the associated hormonal changes, which can cause the ovarian ligaments to relax and increase the risk of torsion. According to statistics, pregnancy is the cause of 20% of torsion cases.
- Ovarian stimulation in fertility treatments (ovarian hyperstimulation).
- Ovarian ligaments that are too long or congenital anatomical abnormalities that allow the ovary to twist.
- Pelvic trauma or postoperative adhesions.
- Polycystic ovary syndrome , as the presence of multiple small cysts can alter the weight and size of the ovaries and the elasticity of the supporting tissues, increasing susceptibility to torsion.
- History of ovarian torsion, as anatomical changes and the formation of postoperative adhesions increase the risk of recurrence.
Symptoms of ovarian torsion
Symptoms of ovarian torsion usually come on suddenly and may initially include:
- Intense, sharp, one-sided pelvic pain (left or right).
- Frequent nausea and vomiting.
- Fever, sweating and altered general condition.
- Abdomen tender to touch or abdominal cramps.
- Occasionally, light vaginal bleeding.
As more time passes since the twist, the pain may radiate to the back or thigh, and bleeding in the abdomen may occur.
The intensity and duration of symptoms may vary, and fever may persist for several weeks, but severe pain, at a level never felt before, is a constant and a clear sign that medical consultation is necessary.
Diagnosis for ovarian torsion
Suspicion of ovarian torsion most often arises based on symptoms and clinical examination, and the diagnosis is confirmed by imaging investigations.
There are also some situations in which the condition is confirmed with certainty only during surgery, because time directly influences the chances of saving the ovary and emergency intervention may be necessary.
Clinical examination and history
The first step of the consultation consists of a clinical examination and a discussion through which the doctor seeks to learn as much as possible about the patient's medical history.
Physical evaluation involves palpating the lower abdomen and pelvic area to identify the location of the pain, its intensity, and the presence of signs of peritoneal inflammation. In order to make a diagnosis, the patient is asked questions about the sudden onset of pain and associated symptoms such as nausea or vomiting.
The doctor also pays attention to tenderness to palpation and signs of muscle defense, which are key indicators for differential diagnosis. They can help rule out other acute causes such as appendicitis or renal colic, which can have similar manifestations.

Transvaginal Doppler ultrasound for ovarian torsion
Transvaginal ultrasound is the main investigation in diagnosing ovarian torsion, and color Doppler analysis is a specialized imaging technique for evaluating blood flow in the ovary.
This type of investigation allows for detailed visualization of the pelvic organs, possible specific changes such as ovarian enlargement, the presence of cysts, ovarian masses or rotated adnexal formations, as well as possible changes in ovarian vascularization. In other words, if blood flow is reduced or absent in an ovary, this will be seen on transvaginal Doppler ultrasound.
However, the presence of apparently normal flow does not completely rule out the diagnosis, especially in the early stages. There are cases where the condition exists even if blood flow is present, as the torsion may be partial or intermittent.
Additional imaging investigations for ovarian torsion
Additional investigations may be used in the diagnostic process to rule out other possible causes of acute abdominal pain.
Computed tomography (CT) or magnetic resonance imaging (MRI) allow for a closer evaluation of pelvic structures to differentiate from other abdominal conditions. Measurement of inflammatory markers through blood tests, pregnancy tests, and urine tests may also be recommended.
However, the definitive diagnosis is often confirmed intraoperatively, during laparoscopy. This procedure allows direct visualization of the twisted ovary and at the same time offers the possibility of immediate treatment.
Treatment for ovarian torsion
Ovarian torsion is a surgical emergency, and the treatment procedure must be started as quickly as possible to increase the chances of saving the ovary and the function it performs.
Laparoscopic surgery is the standard intervention method, the purpose of which is to restore blood circulation and prevent irreversible damage to the ovarian tissue. The procedure is minimally invasive and allows both confirmation of the diagnosis and immediate treatment.
When laparoscopy is not feasible, for example when there are large ovarian masses that need to be removed or when severe complications occur, a laparotomy may be performed. The incision is larger in the abdomen, and the surgeon gains better access and visibility of the pelvic structures.
Preoperatively, intravenous analgesics may be administered for rapid pain relief. Antibiotic treatment may also be recommended if there is a risk of infection or if the ovarian torsion is complicated by ischemic changes.
During the intervention, the surgeon performs detorsion of the ovary to restore blood flow and assesses the vitality of the ovarian tissue to determine the next step:
- Ovary salvage, which is possible if there are no signs of necrosis and consists of repositioning the ovary normally, is also the ideal situation, especially in young patients.
- Oophoropexy, a procedure in which the ovary is fixed to reduce the risk of torsion recurring.
- Ovariectomy, i.e. removal of the compromised ovary, when the ovarian tissue is severely damaged and necrotic.
After the intervention, postoperative monitoring is necessary for recovery, to assess ovarian function, and to protect long-term fertility.
Complications of ovarian torsion
If left untreated, ovarian torsion can have consequences for reproductive health and the ability to become pregnant, the severity of which depends largely on the duration of the interruption of blood flow. The most common complications include:
- Ovarian necrosis, i.e. tissue death due to lack of oxygen, a situation in which the ovary can no longer be saved and must be surgically removed.
- Secondary infertility, if ovarian function is significantly impaired or if removal of the ovary is necessary.
- Pelvic infection.
- Peritonitis (inflammation of the peritoneum), in severe cases.
- The risk of recurrence in the same ovary (especially if oophoropexy was not performed) or in the opposite ovary.
Ovarian torsion and menstruation
Menstruation is not a direct cause of ovarian torsion, but the pain specific to the condition can be confused with menstrual cramps due to similar location and manifestations. In this case, the intensity of symptoms and response to treatment can be useful indicators to differentiate the two types of pain.
During menstruation, the pain caused by torsion is usually much more intense and unilateral. Unlike menstrual cramps, this type of pain does not improve with common anti-inflammatory drugs and an intimate care routine with gentle menstrual products . If pelvic pain persists for more than 24 hours and is accompanied by nausea or fever, an ultrasound is necessary to confirm or rule out ovarian torsion.
Ovarian torsion can also be influenced by other phases of the menstrual cycle. During the premenstrual period, the ovaries may be larger due to functional cysts, increasing the risk of cyst torsion. After menstruation, torsion can occur in the context of ovulation or a persistent cyst. And in some cases, menstruation can be delayed if ovarian function is impaired.
When to go to the emergency room for ovarian torsion
Saving a twisted ovary directly depends on how quickly surgical intervention is performed, so any suspicion of ovarian torsion is an emergency and you should see a doctor at the first signs. Seek immediate medical attention if you experience:
- Sudden and severe, unilateral pelvic pain.
- Persistent nausea and vomiting.
- Fever, dizziness, rapid pulse, or cold sweats.
Frequently asked questions about ovarian torsion (FAQ)
Are you worried about the consequences of ovarian torsion and need more information? Below you will find clear and quick answers to the most common questions patients have about the risk of recurrence, recovery after surgery, and the effects of ovarian torsion on fertility.
Can ovarian torsion be prevented?
There is no surefire method of prevention, but monitoring ovarian cysts and treating gynecological conditions can reduce the risk of ovarian torsion. In patients who have been previously diagnosed, the risk of a new torsion can be reduced by oophoropexy.
Can ovarian torsion occur during pregnancy?
Yes, ovarian torsion is possible, especially in the first trimester, when hormonal changes can cause the ovary to enlarge and the ligaments to relax. Approximately 20% of cases occur during pregnancy.
What happens if ovarian torsion treatment is delayed?
The longer surgery is delayed and blood flow to the ovary is interrupted, the greater the risk of ovarian inflammation and necrosis, which in turn may lead to the need for removal of the ovary and possible effects on fertility.
Can one live normally with only one ovary?
A single functioning ovary is, in most cases, sufficient to maintain the menstrual cycle and achieve pregnancy.
How does pain manifest in ovarian torsion?
The pain specific to ovarian torsion comes on suddenly and is felt intensely, on one side. It may be accompanied by nausea and vomiting and is not significantly relieved by common painkillers.
Can ovarian torsion recur after surgery?
Yes, recurrence is possible after surgical treatment for ovarian torsion, but oophoropexy (fixation of the ovary) can reduce this risk.
How long does recovery take after ovarian torsion surgery?
Recovery from laparoscopy is generally quick. Most patients can resume their normal activities within one to two weeks.
What tests confirm the diagnosis of ovarian torsion?
Transvaginal Doppler ultrasound is the primary method for diagnosing ovarian torsion, which may be accompanied by blood, urine, and pregnancy tests, as well as CT or MRI scans. In some cases, the diagnosis is definitively confirmed only during laparoscopy.
Is fertility affected after ovarian torsion?
If the ovary is saved, fertility is not affected by its torsion. There may be difficulty achieving pregnancy if the compromised ovary needs to be removed, but in general the healthy ovary can continue to perform its ovulatory function, preventing infertility.
What are the alarm symptoms in teenagers for ovarian torsion?
Sudden, severe, and persistent pelvic pain on one side, nausea, vomiting, and fever should be evaluated immediately, even in adolescents with no known gynecological history.
Photo source: Pexels.com

















and happily breaking taboos!





